What is Adenomyosis?
Adenomyosis is a common, non-cancerous condition of the uterus. It occurs when the tissue that normally lines the inside of the uterus (the endometrium) begins to grow into the muscular wall of the uterus (the myometrium).
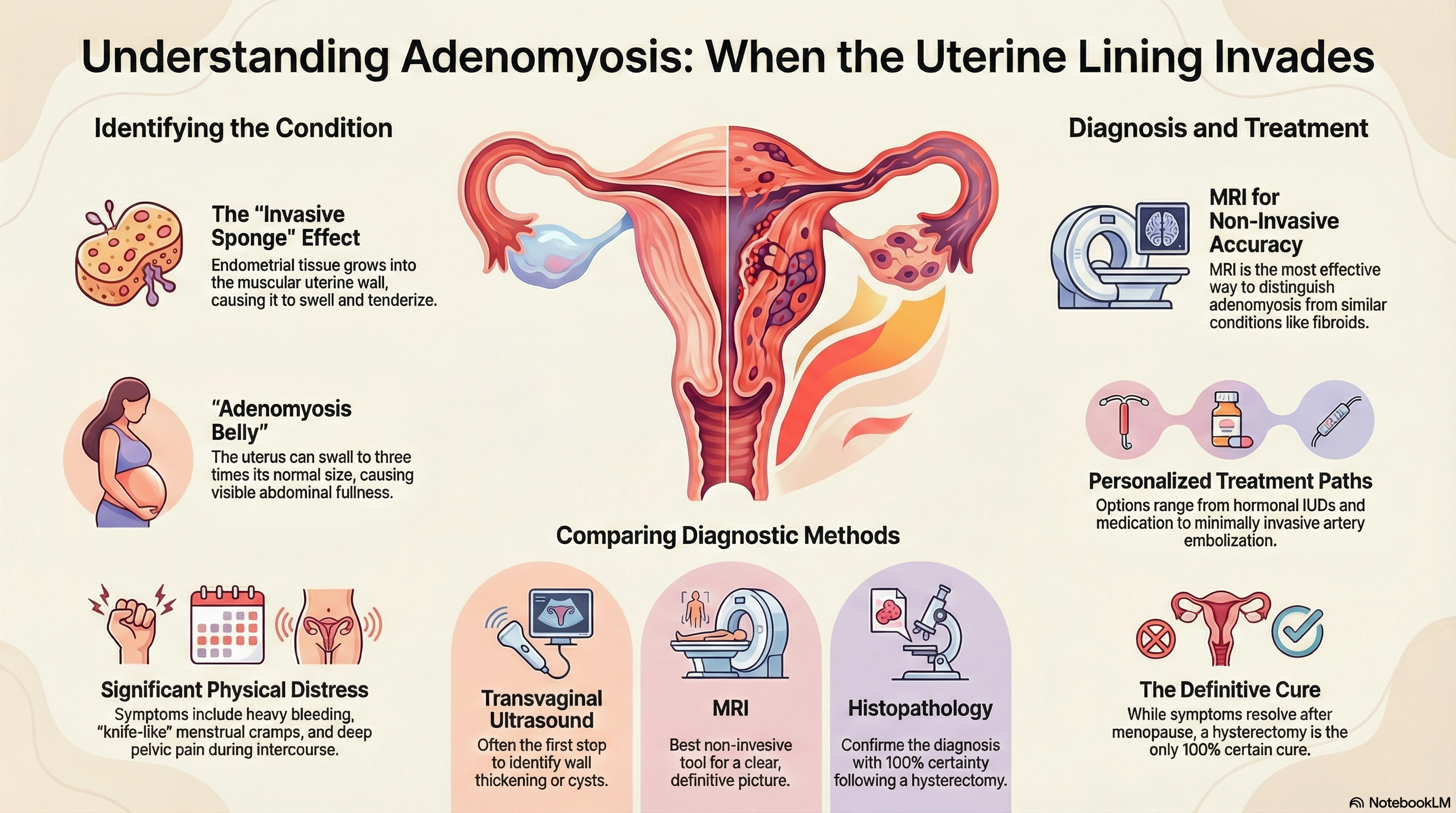
Think of the uterine wall like a thick, muscular sponge. Normally, the lining stays on the inner surface. In adenomyosis, this lining tissue invades the "sponge" itself. Because this misplaced tissue continues to behave normally—thickening and bleeding during your menstrual cycle—but has no way to escape the muscle, it causes the uterine wall to swell. This leads to an enlarged, tender uterus and significant pain. While historically associated with women over 40, improved imaging now identifies this condition frequently in younger women of reproductive age.
Causes of Adenomyosis
The exact cause of adenomyosis is not yet fully understood, but it is known to be an estrogen-dependent condition, meaning it thrives on the female hormone estrogen. Several leading theories include:
Invasive Tissue Growth This is the most widely accepted theory. It suggests that endometrial cells directly invade the muscle wall, often triggered by "wounds" or disruptions to the boundary between the lining and the muscle. This explains why uterine procedures like C-sections or D&Cs (dilation and curettage) increase risk.
Developmental Origins Some experts believe the tissue was misplaced in the uterine muscle during fetal development, long before a woman is even born.
Uterine Inflammation Inflammation of the uterine lining during childbirth or surgery may break down the normal barriers, allowing cells to migrate into the muscle.
Risk Factors
-
Age: Most commonly diagnosed in women in their 40s and 50s due to long-term estrogen exposure.
-
Childbirth: Having had at least one pregnancy increases the likelihood.
-
Prior Surgery: C-sections, fibroid removals, or other uterine surgeries.
Symptoms of Adenomyosis
While approximately one-third of patients have no symptoms at all, many experience significant physical distress.
Common Physical Signs
-
Heavy Menstrual Bleeding: Periods that are abnormally heavy or last longer than a week, sometimes leading to anemia.
-
Severe Cramping: Known as dysmenorrhea, this pain can be sharp, "knife-like," or a deep, constant ache.
-
Chronic Pelvic Pain: A persistent feeling of pressure or pain in the pelvic region, even when not on your period.
-
Pain During Intercourse: Deep pelvic pain during or after sex.
-
"Adenomyosis Belly": The uterus can become two to three times its normal size, leading to a visible swelling or a sense of fullness in the lower abdomen.
Fertility and Pregnancy Adenomyosis is increasingly linked to infertility, as it can interfere with how an egg implants. It is also associated with an increased risk of miscarriage and other obstetric complications.
Diagnosis of Adenomyosis
Diagnosing adenomyosis can be tricky because its symptoms are very similar to uterine fibroids or endometriosis (where tissue grows outside the uterus).
Clinical Examination During a pelvic exam, a doctor may feel that the uterus is enlarged, "boggy" (soft), or tender to the touch.
Imaging Tests
-
Transvaginal Ultrasound: Usually the first step, where a probe is used to look for a thickened uterine wall or small cysts within the muscle.
-
MRI (Magnetic Resonance Imaging): This is the most effective non-invasive way to diagnose the condition. It provides a clear picture that helps doctors distinguish adenomyosis from fibroids.
Histopathology Currently, the only way to confirm adenomyosis with 100% certainty is for a pathologist to examine the uterus under a microscope after it has been surgically removed (hysterectomy).
Treatment of Adenomyosis
Treatment plans are personalized based on the severity of symptoms and whether the patient wishes to maintain fertility.
Managing Symptoms with Medication
-
Anti-inflammatory Drugs: NSAIDs like ibuprofen can help with mild pain and reduce blood flow.
-
Hormonal Suppression: This is the most common approach. Options include the levonorgestrel-releasing IUD (like Mirena), birth control pills, or progestin injections. These thin the uterine lining and stop the bleeding cycle.
-
GnRH Agonists: These medications induce a temporary "medical menopause" to shrink the tissue, though they are usually only used short-term.
Minimally Invasive Procedures
-
Uterine Artery Embolization (UAE): Tiny particles are injected into the blood vessels to cut off the blood supply to the adenomyosis, causing it to shrink.
-
Endometrial Ablation: This destroys the thin lining of the uterus to reduce heavy bleeding, but it may not help with deep muscular pain.
Surgical Options
-
Adenomyomectomy: Surgery to remove only the affected tissue while keeping the uterus intact. This is complex and carries a risk of the condition returning.
-
Hysterectomy: The surgical removal of the uterus. This is the only definitive cure for adenomyosis.
Prevention of Adenomyosis
Because the exact cause of adenomyosis is unknown and tied to hormonal and developmental factors, there is no guaranteed way to prevent it. However, you can manage your risks and uterine health.
Early Intervention Seeking help at the first sign of abnormally heavy or painful periods can lead to earlier diagnosis and the use of hormonal treatments that may slow the progression of the disease.
Surgical Awareness Being aware that uterine surgeries (like C-sections) can increase risk allows you and your doctor to monitor your pelvic health more closely following these procedures.
Hormonal Balance Since the condition is fueled by estrogen, maintaining a healthy lifestyle that supports hormonal balance may be beneficial. It is important to note that symptoms typically resolve naturally after menopause, when estrogen levels drop significantly.