What is Back Pain?
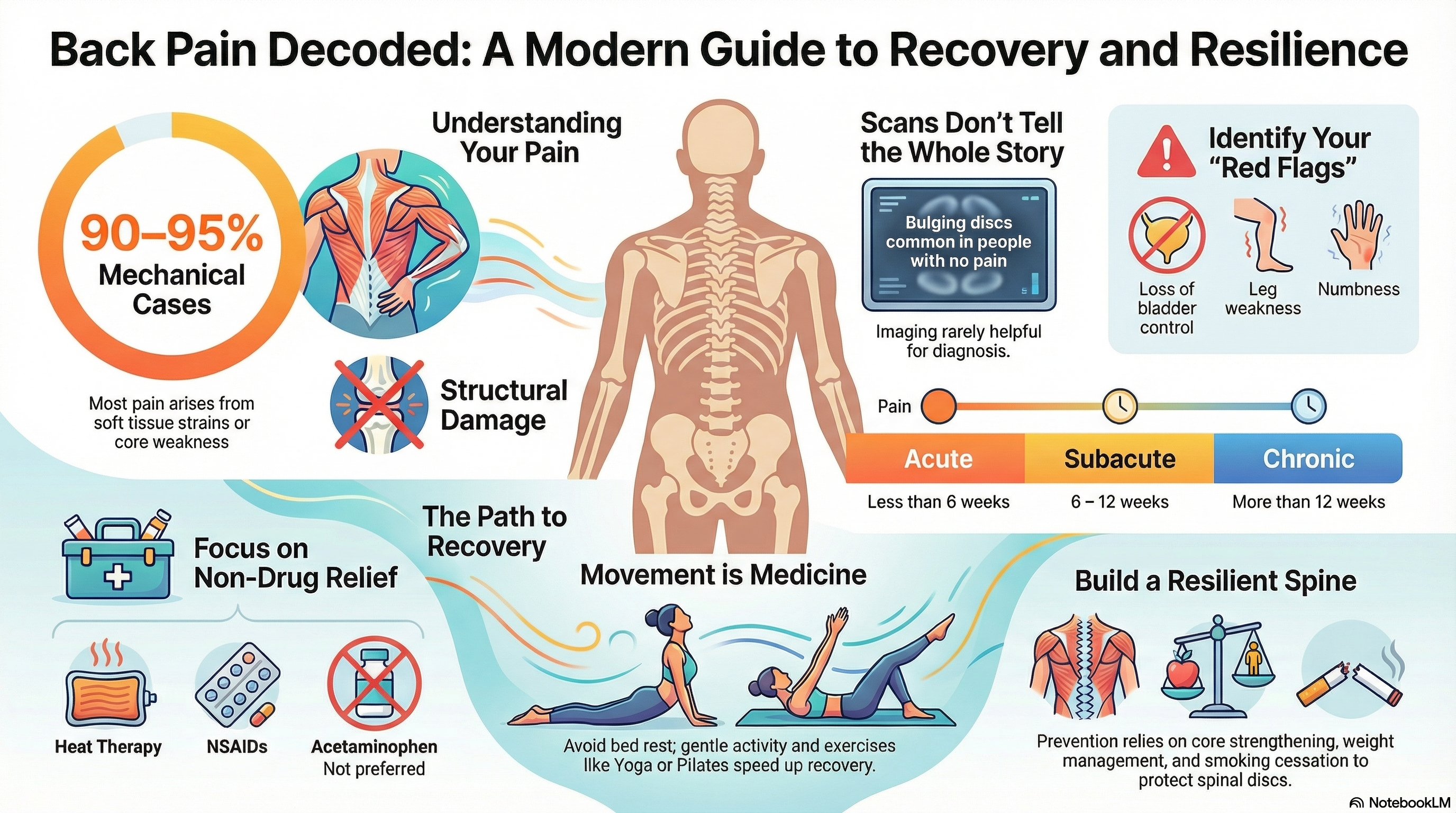
Back pain is categorized primarily by how long it lasts. Acute pain lasts less than 6 weeks and is often the result of a sudden strain. Subacute pain lasts 6–12 weeks, while Chronic pain persists for more than 12 weeks.
In the majority of cases, imaging like X-rays or MRIs cannot pinpoint a single "pain generator." This is because many findings on a scan—such as bulging discs or arthritis—are common in people with no pain at all. Consequently, 2026 medical guidelines emphasize that back pain is often a complex interaction of biological factors (muscle or ligament strain), psychological factors (stress or fear of movement), and social factors (work environment).
Causes of Back Pain
Back pain is broadly divided into two categories based on the cause:
Non-Specific/Mechanical Pain (90–95% of cases) This is pain arising from the muscles, ligaments, or joints of the spine. Common triggers include:
-
Soft tissue strains or sprains.
-
Degenerative changes (wear and tear) in the discs or facet joints.
-
Poor "spine endurance" or core weakness.
Specific/Structural Causes (5–10% of cases) These are conditions with a clear anatomical cause, such as:
-
Disc Herniation: When a disc presses on a nerve, often causing "sciatica" (pain radiating down the leg).
-
Spinal Stenosis: Narrowing of the spaces within the spine, common in adults over 65.
-
Fractures: Often linked to osteoporosis or significant trauma.
-
Inflammatory Conditions: Such as axial spondyloarthritis.
Symptoms of Back Pain
The symptoms you experience can help determine the source of the pain and whether it is mechanical or nerve-related.
-
Localized Ache: Dull, aching pain strictly in the lower back, often worse with certain movements.
-
Radiculopathy (Sciatica): Sharp, shooting pain, numbness, or tingling that travels from the back down into the buttock and leg.
-
Stiffness: Difficulty standing up straight or a limited range of motion, especially in the morning.
-
Muscle Spasms: Intense, involuntary contractions of the back muscles.
Red Flags: When to See a Doctor Immediately While rare, some symptoms indicate a medical emergency (such as Cauda Equina Syndrome):
-
Loss of bladder or bowel control.
-
"Saddle anesthesia" (numbness in the groin or buttocks).
-
Sudden, progressive weakness in the legs or "foot drop."
-
Pain accompanied by fever, unexplained weight loss, or a history of cancer.
Diagnosis of Back Pain
Diagnosis focuses on a thorough history and physical exam rather than immediate imaging.
-
Physical Examination: Your doctor will check your reflexes, muscle strength, and how you respond to specific movements. The "straight-leg raise" test is a common tool used to check for disc-related nerve irritation.
-
The Role of Imaging: Routine X-rays or MRIs are not recommended for non-specific back pain. Imaging is generally reserved for cases where "red flags" are present or when pain has not improved after 6–12 weeks of conservative treatment.
-
Clinical History: Your doctor will ask about the timing of the pain, your activity levels, and any history of trauma to rule out serious pathology.
Treatment of Back Pain
Current 2026 guidelines favor non-drug treatments as the first-line defense against back pain.
First-Line Strategies
-
Stay Active: Contrary to old advice, bed rest is harmful and can delay recovery. Gentle movement is essential.
-
Education and Reassurance: Understanding that most back pain is not caused by permanent damage helps reduce the "fear-avoidance" that can lead to chronic pain.
-
Heat Therapy: Applying heat can help relax spasming muscles and reduce acute pain.
-
Specialized Exercise: Yoga, Pilates, and the "McGill Big 3" (Curl-up, Side Plank, and Bird-dog) are highly recommended to build spine endurance.
Pharmacologic and Procedural Options
-
Medications: NSAIDs (like ibuprofen or naproxen) are the first-line choice for medication. Acetaminophen is generally no longer recommended for back pain due to a lack of efficacy. Second-line options for chronic pain may include duloxetine.
-
Complementary Care: Acupuncture, massage, and spinal manipulation can provide short-term relief.
-
Surgery: Surgery is only necessary for about 1–5% of people, typically those with progressive nerve damage or disabling sciatica that has not responded to months of non-surgical care.
Prevention of Back Pain
Preventing back pain is more about building a resilient body than following strict "rules" about posture.
-
Exercise Regularly: Combining cardiovascular health with core-strengthening exercises is the most effective way to prevent future episodes.
-
Smoking Cessation: Smoking is a major risk factor for back pain because it impairs blood flow to the spinal discs, accelerating degeneration.
-
Safe Lifting: While "perfect" posture is a myth, using your legs and keeping loads close to your body during heavy lifting reduces sudden mechanical strain.
-
Weight Management: Reducing excess body weight decreases the constant load on the lumbar spine.
-
Ergonomics: Ensure your workstation allows for frequent position changes throughout the day.