What is Chronic Fatigue Syndrome?
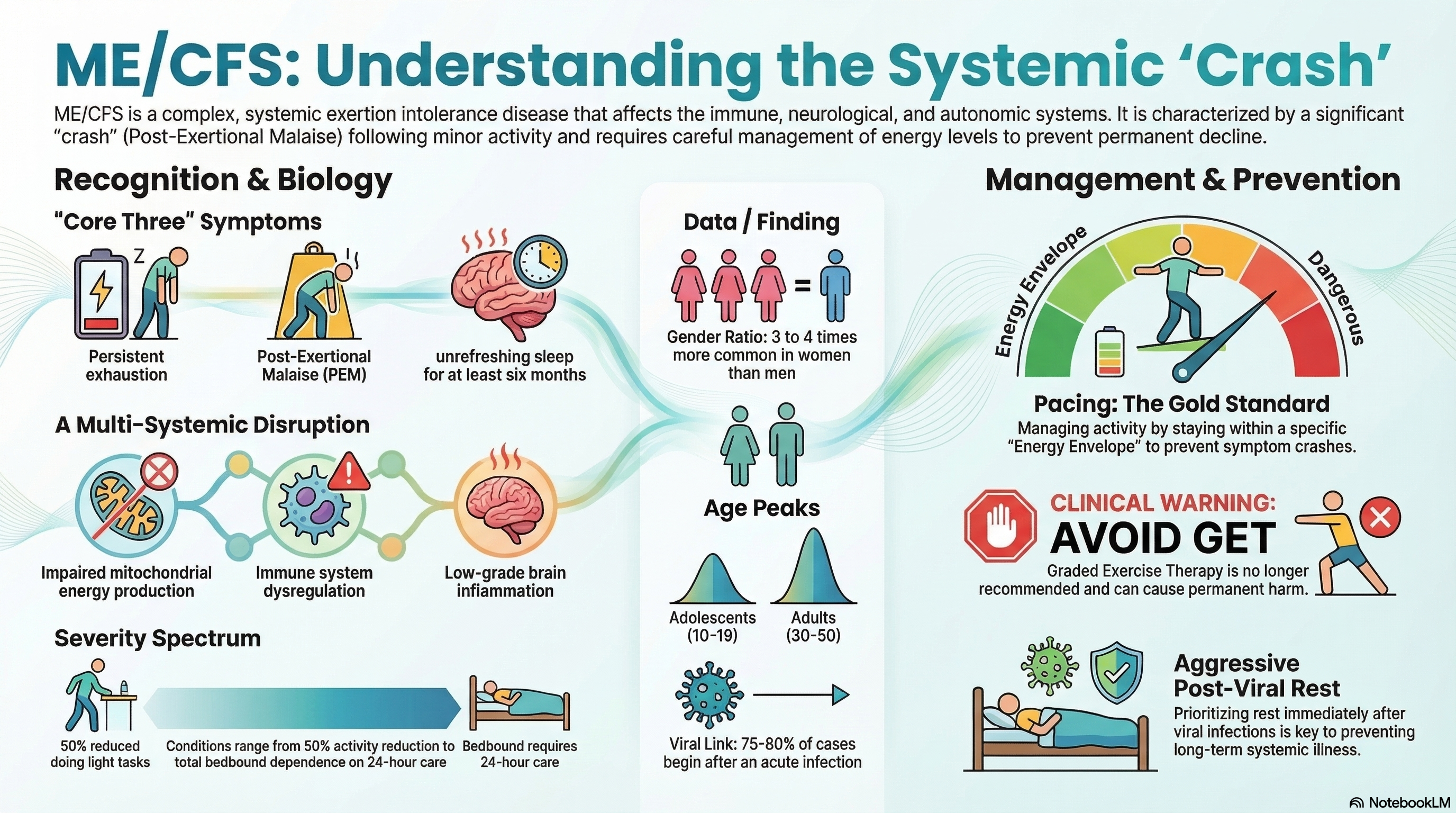
ME/CFS is more than just "being tired." It is a systemic exertion intolerance disease that affects the immune, neurological, and autonomic systems. The hallmark of the condition is Post-Exertional Malaise (PEM)—a formal term for a "crash" where symptoms worsen significantly after physical, mental, or emotional effort that would have been trivial before the illness.
The severity of the condition varies widely:
-
Mild: At least a 50% reduction in pre-illness activity levels.
-
Moderate: Mostly housebound; unable to work or attend school regularly.
-
Severe: Mostly or entirely bedbound; requires assistance with basic self-care.
-
Very Severe: Entirely bedbound and dependent on 24-hour care; often requires tube feeding and has total intolerance to light and sound.
Causes of Chronic Fatigue Syndrome
While the exact cause remains under investigation, 2024–2025 research suggests it is a multifactorial condition often triggered by a major "insult" to the immune system.
-
Viral and Bacterial Triggers: About 75–80% of cases begin after an acute infection. Common triggers include the Epstein-Barr virus (mononucleosis), Ross River virus, and increasingly, SARS-CoV-2 (COVID-19). Research indicates an overlap of 50–70% between Long COVID and ME/CFS.
-
Immune Dysregulation: Patients often show low Natural Killer (NK) cell function and chronic "cytokine storms," where the body remains in a permanent state of high-alert inflammation.
-
Metabolic Dysfunction: Emerging evidence shows "impaired energy metabolism" at a cellular level. The mitochondria (the power plants of your cells) fail to produce enough ATP, the body's primary energy currency.
-
Neuroinflammation: Recent neuroimaging studies from Stanford (2023) and the NIH (2024) have found evidence of low-grade inflammation in the brain.
-
Demographics: The disease is roughly 3 to 4 times more common in women than men. While it affects all ethnicities, the age of onset typically peaks in two groups: adolescents (10–19 years) and adults (30–50 years).
Symptoms of Chronic Fatigue Syndrome
The symptoms of ME/CFS are widespread and can fluctuate in intensity. To meet the modern diagnostic standard, a patient must experience the "Core Three" symptoms for at least six months.
The Core Three Symptoms:
-
Exhaustion: A profound, persistent fatigue that is not the result of unusual exertion and is not relieved by sleep or rest.
-
Post-Exertional Malaise (PEM): A delayed (12–48 hours) "crash" after activity that can last for days or weeks.
-
Unrefreshing Sleep: Feeling just as tired after a full night's sleep as before going to bed.
Additional Common Symptoms:
-
Cognitive Impairment ("Brain Fog"): Problems with memory, concentration, and processing information.
-
Orthostatic Intolerance: Feeling dizzy, lightheaded, or faint when standing up (often diagnosed as POTS—Postural Orthostatic Tachycardia Syndrome).
-
Pain: Chronic headaches, muscle aches, and multi-joint pain without redness or swelling.
-
Immune Symptoms: Frequent sore throats, tender lymph nodes in the neck or armpits, and new sensitivities to light, noise, or chemicals.
Diagnosis of Chronic Fatigue Syndrome
There is currently no single blood test to "prove" you have ME/CFS. Instead, diagnosis is "clinical," based on a thorough medical history and the exclusion of other treatable conditions like thyroid disease, anemia, or sleep apnea.
-
Clinical Criteria: Most specialists now use the 2015 National Academy of Medicine criteria, which focus on the core symptoms of PEM, unrefreshing sleep, and cognitive or standing issues.
-
Exclusionary Testing: Doctors will run extensive blood panels to rule out other diseases. In some specialized clinics, a 2-day CPET (Cardiopulmonary Exercise Test) is used to objectively document the drop in energy production on the second day—the biological proof of PEM.
-
Autonomic Testing: A "Tilt Table Test" or a "NASA Lean Test" is used to diagnose orthostatic intolerance.
-
Biomarker Research: While not yet standard, 2024 studies are looking at "itaconic acid" levels and T-cell exhaustion as potential future diagnostic markers.
Treatment of Chronic Fatigue Syndrome
There is currently no FDA-approved cure for ME/CFS. Treatment focuses strictly on managing symptoms and preventing the "crashes" that lead to permanent decline.
The Gold Standard: Pacing Pacing is the most important management tool. It involves staying within your "Energy Envelope" and stopping activity before you feel tired. Unlike other illnesses, "pushing through" the pain in ME/CFS is clinically proven to be harmful.
Medications and Supplements:
-
Low-Dose Naltrexone (LDN): Used at very low doses (1–4.5 mg) to reduce neuroinflammation and pain.
-
Low-Dose Aripiprazole (Abilify): Emerging 2023–2025 evidence suggests very low doses (0.25–2 mg) can improve brain fog and energy in some patients.
-
Pyridostigmine (Mestinon): Often used to help with standing issues and muscle weakness.
-
Sleep Supports: Non-habit-forming sleep aids are used to improve sleep quality.
Important Warning: Older treatments like "Graded Exercise Therapy" (GET) have been removed from clinical guidelines (including the UK's NICE 2021 update) because they are proven to cause permanent harm to ME/CFS patients.
Prevention of Chronic Fatigue Syndrome
Because ME/CFS is often triggered by an infection, prevention centers on supporting the immune system and proper recovery from viral illnesses.
-
Rest During Acute Illness: The best way to prevent a post-viral syndrome like ME/CFS is to rest aggressively during and immediately after a viral infection (like the flu or COVID-19). Avoid the "pushing through" mentality during recovery.
-
Early Intervention: If you experience symptoms of PEM (crashing after activity) following a virus, adopting a pacing strategy immediately may prevent the condition from becoming severe or permanent.
-
Managing Stress: Chronic high stress combined with an infection is a common precursor to the disease; managing physiological stress can help maintain immune resilience.
-
Vaccination: Preventing the initial infections known to trigger ME/CFS (such as influenza or COVID-19) is a primary preventive measure.