What is Athlete's Foot?
Athlete's foot is a superficial fungal infection that typically begins between the toes. The fungi feed on keratin, a protein found in the outer layer of your skin, hair, and nails. Because these fungi do not invade living tissue, they stay on the very surface of the skin, causing inflammation and scaling.
There are four main ways the infection presents itself:
-
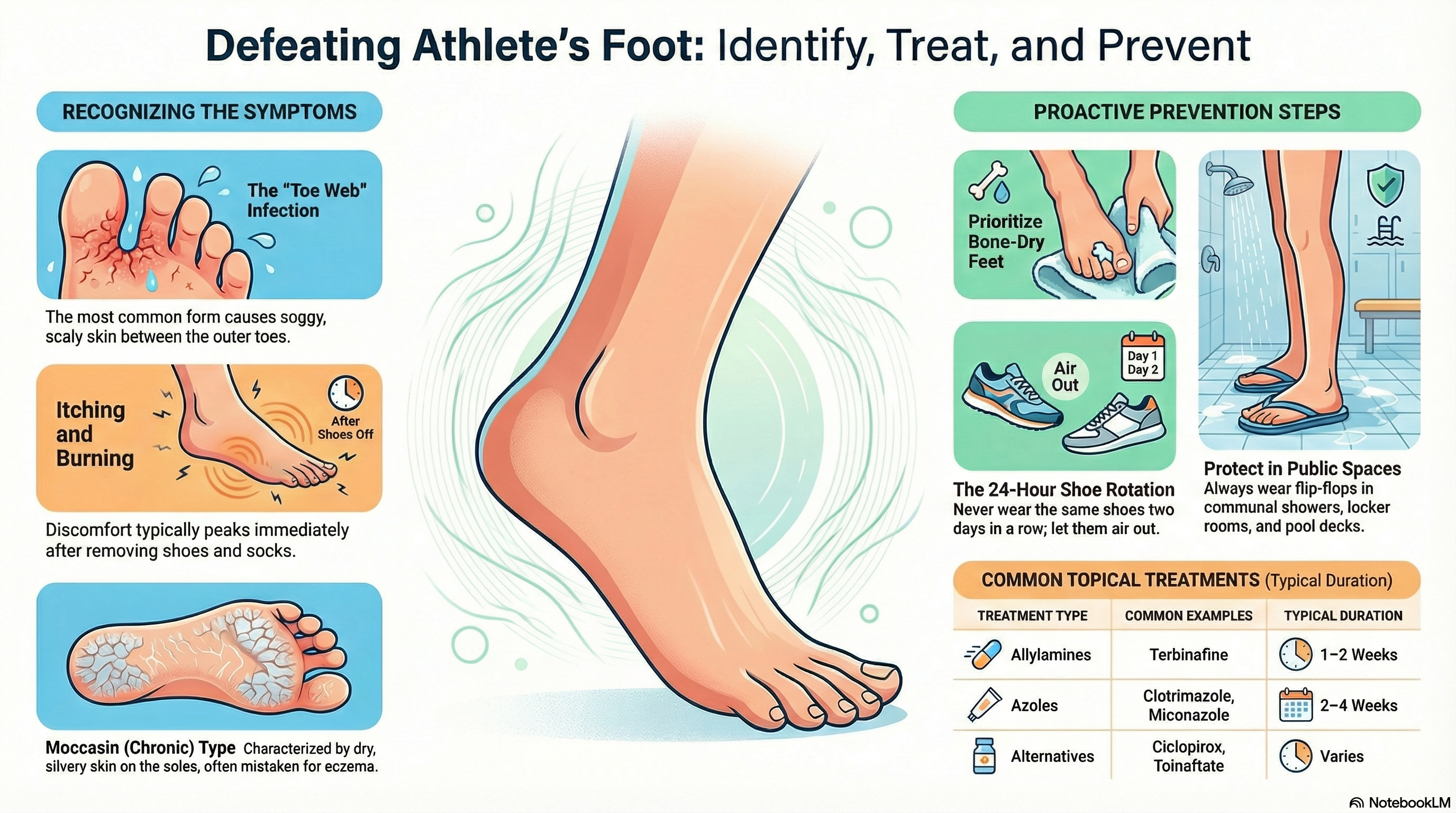
Interdigital (Toe Web): The most common type. It usually starts between the fourth and fifth toes, causing the skin to look white, soggy (macerated), and scaly.
-
Moccasin (Chronic): This involves the soles, heels, and sides of the feet. It looks like dry, thickened, or silvery skin and is often mistaken for simple dry skin or eczema.
-
Vesicular (Inflammatory): This type causes sudden outbreaks of itchy blisters, usually on the instep or arch of the foot.
-
Ulcerative: The most severe form, characterized by open sores and peeling skin, often complicated by a secondary bacterial infection.
Causes of Athlete's Foot
The primary cause of athlete's foot is a group of fungi, with Trichophyton rubrum being the most frequent culprit. You can contract the fungus through direct contact with an infected person or by touching contaminated surfaces.
Common Triggers and Environments:
-
Communal Areas: Walking barefoot in locker rooms, public showers, and swimming pool decks.
-
Footwear: Wearing tight, heavy, or non-breathable shoes (like work boots or sneakers) that trap sweat against the skin.
-
Moisture: Keeping your feet wet for long periods or failing to dry thoroughly between your toes after a shower.
-
Shared Items: Using towels, socks, or shoes that have been used by someone with the infection.
Who is at Risk? While anyone can get it, certain groups are more susceptible, including males, the elderly, and individuals with weakened immune systems or diabetes. Athletes, military personnel, and people who work in hot, humid environments have higher rates of the condition.
Symptoms of Athlete's Foot
The symptoms of athlete's foot vary depending on the type of infection you have, but most people experience a combination of the following:
-
Itching and Burning: This is the most common complaint, often feeling worst immediately after you take off your shoes and socks.
-
Scaling and Peeling: The skin may flake off or appear cracked (fissures).
-
Maceration: Between the toes, the skin may look white, soft, and "soggy."
-
Blisters: Small, itchy, fluid-filled bumps that may ooze or crust over.
-
Odor: A foul smell can develop, especially if bacteria have also begun to grow in the area.
-
Discoloration: The affected skin may appear red, gray, or even purple depending on your skin tone.
Diagnosis of Athlete's Foot
A doctor can often diagnose athlete's foot simply by looking at your feet and asking about your symptoms. However, since other conditions like psoriasis or contact dermatitis can look similar, they may use specific tests to confirm the fungus.
-
KOH Prep: The doctor gently scrapes a small sample of the scaly skin and places it in a potassium hydroxide (KOH) solution. This dissolves the skin cells but leaves the fungal elements visible under a microscope.
-
Fungal Culture: A skin sample is placed in a special laboratory dish to see if the fungus grows. This can take several weeks but identifies the exact type of fungus.
-
Wood's Lamp: A specialized UV light can sometimes help rule out other types of infections (like erythrasma), though most athlete's foot fungi do not glow under this light.
Treatment of Athlete's Foot
Most cases of athlete's foot can be treated effectively with over-the-counter (OTC) medications, but stubborn or extensive infections may require a prescription.
Topical Treatments (Creams, Sprays, and Powders)
-
Allylamines (e.g., Terbinafine): Often considered the fastest-acting and most effective topical treatments. They usually require 1–2 weeks of use.
-
Azoles (e.g., Clotrimazole, Miconazole): These are common OTC options that typically require 2–4 weeks of twice-daily application.
-
Ciclopirox or Tolnaftate: Other effective alternatives if the first-line treatments don't work.
Oral Medications If the infection is severe, covers the entire "moccasin" area, or has spread to the toenails, your doctor may prescribe oral antifungal tablets like Terbinafine or Itraconazole. These are taken for several weeks and require monitoring of your liver function.
Managing Secondary Infections If the skin is broken and a bacterial infection develops (causing increased pain, redness, or warmth), you may also need a course of antibiotics.
Prevention of Athlete's Foot
Athlete's foot is notorious for coming back. Up to 50% of people will experience a recurrence, so long-term prevention is key.
-
Dry Your Feet: This is the most important step. After bathing, use a separate towel for your feet and make sure the skin between your toes is completely dry.
-
Rotate Your Shoes: Don't wear the same pair of shoes two days in a row. Give them 24 hours to air out and dry completely.
-
Wear Breathable Socks: Choose moisture-wicking materials like wool or specialized synthetics rather than 100% cotton, which stays damp. Change your socks daily.
-
Protect Your Feet in Public: Always wear flip-flops or water shoes in communal showers, locker rooms, and around public pools.
-
Use Antifungal Powder: If you are prone to infection, dusting your feet and the inside of your shoes with antifungal powder daily can prevent the fungus from taking hold.
-
Avoid Sharing: Never share towels, shoes, or socks with others, even family members.