What is Benign Paroxysmal Positional Vertigo (BPPV)?
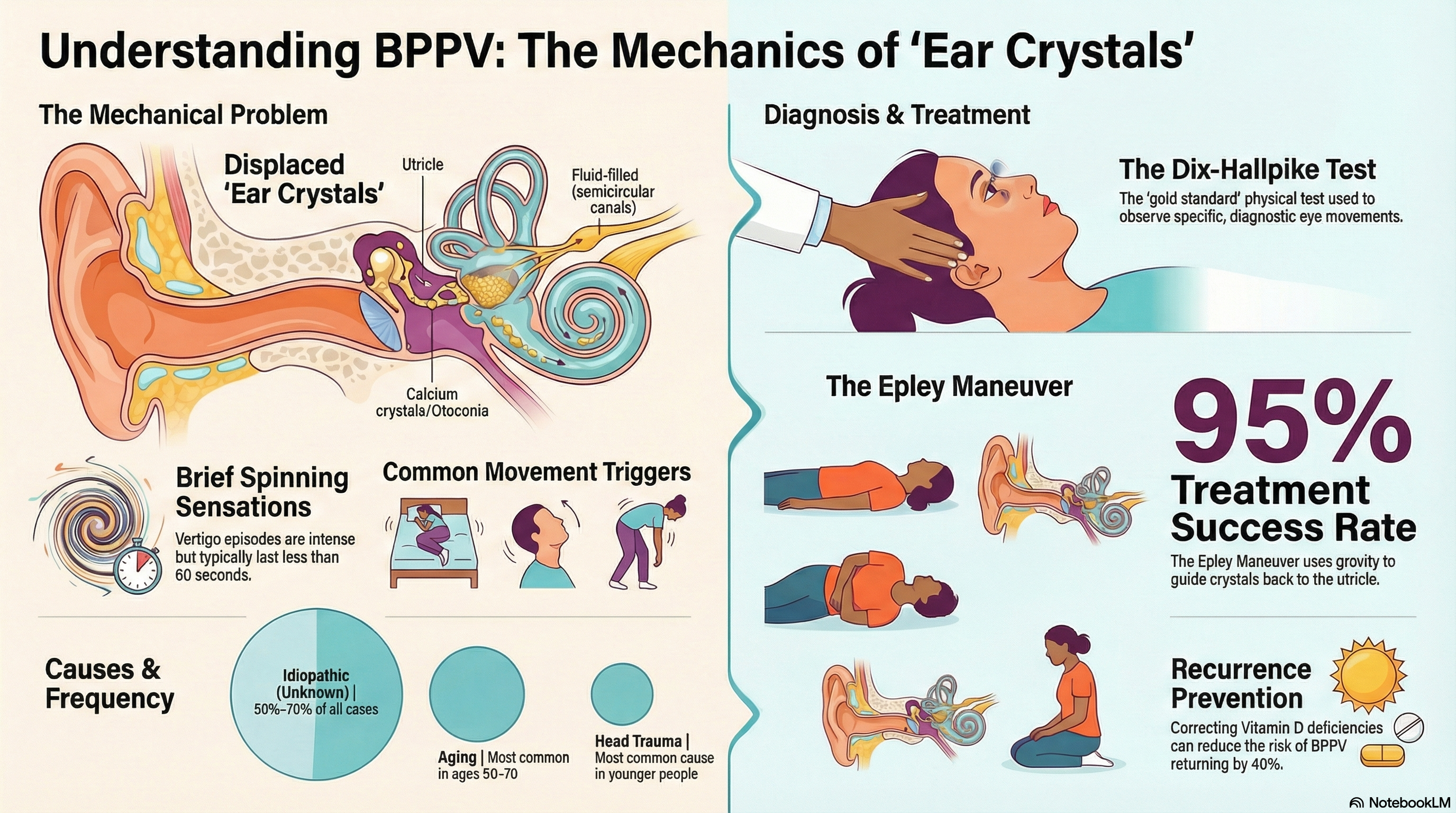
BPPV occurs when tiny "ear crystals" made of calcium carbonate (called otoconia) become dislodged from their normal position in the inner ear's utricle. These crystals migrate into the semicircular canals—the loops in your inner ear that detect head rotation.
Once these crystals are in the canals, they move whenever you change your head position. This movement sends false signals to your brain, making it believe you are spinning when you are actually still. BPPV is "paroxysmal" because it comes in sudden, brief bursts, typically lasting less than one minute.
Causes of Benign Paroxysmal Positional Vertigo (BPPV)
In many cases (about 50–70%), there is no clear cause for why the crystals become dislodged. This is known as "idiopathic" BPPV. However, several factors can trigger the condition:
-
Head Trauma: A fall or blow to the head is the most common identifiable cause, especially in younger people.
-
Aging: The gelatinous membrane that holds the crystals in place naturally degenerates over time, making BPPV most common in people aged 50–70.
-
Prolonged Bed Rest: Lying in one position for a long time (such as during surgery or illness) can allow crystals to settle in the canals.
-
Inner Ear Disorders: Conditions like vestibular neuritis or Meniere's disease can damage the inner ear and dislodge crystals.
-
Medical Conditions: Osteoporosis and Vitamin D deficiency are strongly linked to BPPV because they affect how the body manages the calcium used to form the ear crystals.
Symptoms of Benign Paroxysmal Positional Vertigo (BPPV)
The hallmark of BPPV is vertigo that is triggered by head movement. It does not usually cause constant dizziness.
-
Spinning Sensation: A brief but intense "room-spinning" feeling that usually lasts 10 to 60 seconds.
-
Common Triggers: Rolling over in bed, getting in or out of bed, looking up at a high shelf ("top-shelf vertigo"), or bending forward.
-
Nausea: Many people feel sick to their stomach or may vomit during or after an episode.
-
Imbalance: A lingering sense of being "off" or unsteady on your feet even after the spinning stops.
-
What it is NOT: BPPV does not cause hearing loss, ringing in the ears (tinnitus), or neurological symptoms like fainting or numbness. If you experience these, seek medical attention immediately.
Diagnosis of Benign Paroxysmal Positional Vertigo (BPPV)
BPPV is diagnosed through physical tests that purposely trigger a brief episode of vertigo while a healthcare provider observes your eye movements (nystagmus).
-
Dix-Hallpike Test: This is the "gold standard" for diagnosis. Your provider will quickly move you from a sitting to a lying position with your head turned to the side. If you have BPPV in the posterior canal (the most common type), this will trigger a brief spinning sensation and specific eye movements.
-
Supine Roll Test: This test is used to check for crystals in the horizontal canal, which is less common but requires a different treatment maneuver.
-
Diagnostic Tools: While usually not necessary, some doctors use Video Goggles to see your eye movements more clearly. MRI scans and blood tests are rarely needed unless your doctor suspects a more serious neurological cause for your dizziness.
Treatment of Benign Paroxysmal Positional Vertigo (BPPV)
BPPV is not treated with medication, as pills do not move the crystals back to where they belong. Instead, "repositioning maneuvers" are used to guide the crystals out of the canal and back into the utricle.
-
The Epley Maneuver: This is the most successful treatment, with a success rate of up to 95%. It involves a series of four specific head positions held for about 30–60 seconds each.
-
The Semont Maneuver: An alternative to the Epley, this involves a rapid "swinging" movement from one side of the body to the other. It is often used for patients with neck or back issues that make the Epley difficult.
-
Brandt-Daroff Exercises: These are home-based exercises you can do if your vertigo persists. They involve repeating certain movements to help your brain get used to the dizzy signals (habituation).
-
Vitamin D: If your BPPV keeps coming back, your doctor may check your Vitamin D levels. Supplementing if you are deficient can reduce the risk of recurrence by up to 40%.
Prevention of Benign Paroxysmal Positional Vertigo (BPPV)
While it is difficult to prevent the initial onset of BPPV, you can take steps to reduce the chances of it returning.
-
Manage Underlying Health: Treat conditions like osteoporosis and maintain healthy Vitamin D and calcium levels.
-
Avoid Extreme Head Positions: For a few days after a successful treatment, try to avoid extreme head-tilting (like at the dentist or hair salon).
-
Stay Active: Regular movement helps the vestibular system stay healthy, but avoid prolonged periods of completely flat bed rest if possible.
-
Sleep Position: Some evidence suggests that sleeping with your head slightly elevated (using two pillows) may help prevent dislodged crystals from entering the canals.