What is Chest Pain?
Chest pain is a subjective sensation of discomfort in the chest area that can range from a sharp stab to a dull ache or intense pressure. Because the chest contains the heart, lungs, esophagus, and various muscles and bones, the pain can originate from any of these structures.
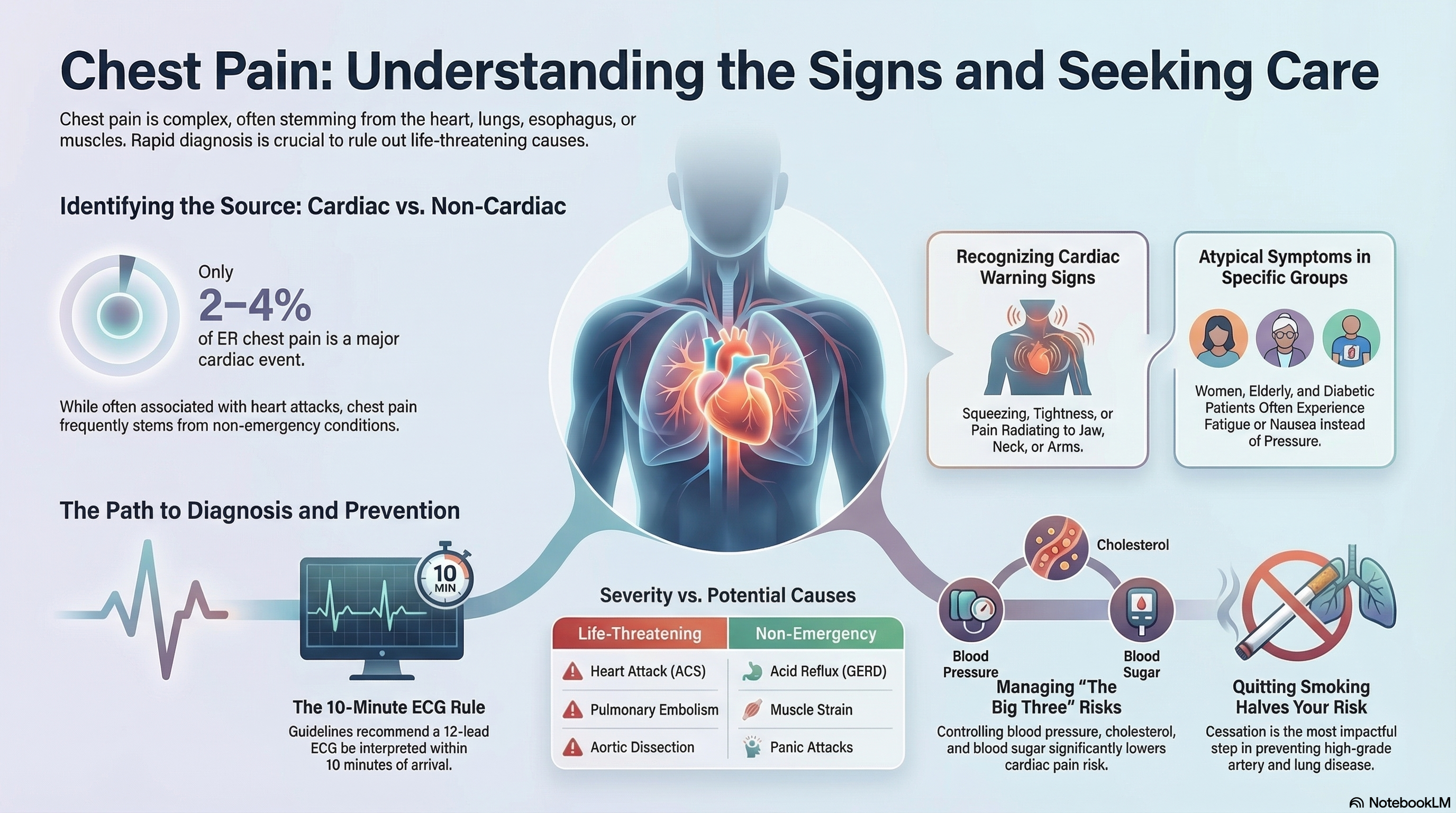
While many people associate chest pain exclusively with a "heart attack," it is a symptom of many different conditions. In the emergency room, only about 2% to 4% of patients presenting with chest pain are found to be having a major cardiac event, though this risk increases significantly with age and underlying health factors.
Causes of Chest Pain
The causes of chest pain are classified by the system they affect. Identifying the cause is a process of elimination, starting with the most dangerous possibilities.
Life-Threatening Causes (Emergency)
-
Acute Coronary Syndrome (ACS): This includes heart attacks and unstable angina, where blood flow to the heart is blocked or severely reduced.
-
Pulmonary Embolism (PE): A blood clot that travels to the lungs.
-
Aortic Dissection: A life-threatening tear in the body's main artery (the aorta).
-
Tension Pneumothorax: A collapsed lung that puts pressure on the heart.
-
Esophageal Rupture: A rare but severe tear in the food pipe, often following forceful vomiting.
Common Non-Emergency Causes
-
Gastrointestinal: The most common cause of non-cardiac pain, including GERD (acid reflux), esophageal spasms, or gallbladder issues.
-
Musculoskeletal: Inflammation of the rib cartilage (costochondritis) or muscle strains in the chest wall.
-
Pulmonary: Pneumonia, asthma, or pleurisy (inflammation of the lung lining).
-
Psychological: Panic attacks and high anxiety can produce physical sensations nearly identical to a heart attack.
Symptoms of Chest Pain
Recognizing the "character" of the pain is vital for determining its source.
Cardiac Warning Signs:
-
Squeezing, tightness, pressure, or a "heavy weight" on the chest.
-
Pain that radiates to the jaw, neck, back, or down one or both arms.
-
Pain triggered by physical exertion or emotional stress.
-
Associated symptoms: Nausea, cold sweats (diaphoretic), dizziness, or extreme shortness of breath.
Non-Cardiac Patterns:
-
Positional: Pain that gets better or worse when you lean forward or change positions.
-
Pleuritic: Sharp, stabbing pain that hurts more when you take a deep breath or cough.
-
Localized: Pain you can point to with one finger or that is painful when you press on the chest wall.
-
Fleeting: Sharp stabs that last only a few seconds.
Group-Specific Differences: Women, elderly patients, and people with diabetes are more likely to experience "atypical" presentations, such as fatigue, nausea, or shortness of breath without classic chest pressure. Additionally, Black patients statistically experience longer diagnostic delays despite having high rates of cardiac etiology.
Diagnosis of Chest Pain
When you seek care for chest pain, doctors use a systematic approach to "risk-stratify" your symptoms.
-
Electrocardiogram (ECG): The most important first step. Guidelines recommend a 12-lead ECG be performed and interpreted within 10 minutes of arrival at a medical facility.
-
Cardiac Troponin (hs-cTn): A blood test that looks for specific proteins released when the heart muscle is damaged. High-sensitivity assays are now the standard, as they can rule out a heart attack more quickly than older tests.
-
Imaging: * Anatomic Testing: Coronary CT Angiography (CCTA) uses a scanner to look for blockages in the heart's arteries.
-
Functional Testing: Stress tests (exercise or medication-induced) observe how the heart behaves under workload.
-
-
Clinical Decision Pathways: Doctors combine your age, history, risk factors (like smoking or diabetes), and lab results to decide if you can be safely discharged or if you need to be admitted.
Treatment of Chest Pain
Treatment is strictly dictated by the underlying cause.
-
For Cardiac Events: Treatments may include "clot-busting" medications, blood thinners like aspirin and heparin, or procedures like an angioplasty to open blocked arteries.
-
For Gastrointestinal Pain: Proton pump inhibitors (PPIs) or antacids are used if acid reflux is the culprit.
-
For Musculoskeletal Pain: Rest and anti-inflammatory medications (NSAIDs) like ibuprofen are usually sufficient.
-
For Pulmonary Embolism: Anticoagulant (blood-thinning) medications are the primary treatment.
-
For Anxiety: Breathing techniques, cognitive therapy, or anti-anxiety medications may be used once a physical cause is ruled out.
Prevention of Chest Pain
Preventing chest pain involves managing the long-term risk factors that lead to heart and lung disease.
-
Manage "The Big Three": Tight control of blood pressure, cholesterol, and blood sugar (diabetes) significantly lowers the risk of cardiac chest pain.
-
Smoking Cessation: Quitting smoking is the most impactful step you can take; it reduces the risk of high-grade artery disease and lung complications by half.
-
Exercise and Weight: Maintaining a healthy weight and engaging in regular physical activity reduces the strain on the heart and helps prevent acid reflux.
-
Screening: If you have a family history of heart disease, speak with your doctor about early screening tests before symptoms ever develop.
-
Healthy Habits: Avoid eating large, spicy meals late at night to prevent GERD-related pain, and use proper form during exercise to avoid chest wall strains.